
Knee and Joint Osteoarthritis: Building an Integrative Pain-Management Plan
Why the patients who manage knee osteoarthritis best are rarely doing one thing, and what a coordinated plan across physiotherapy, chiropractic, and nutrition actually looks like.
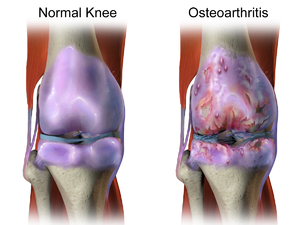
Knee osteoarthritis is one of the most common reasons adults over fifty end up reducing the activities they enjoy. The cartilage that cushions the joint thins over time, the surfaces no longer glide smoothly, and the result is the familiar pattern of stiffness in the morning, ache after sitting, and pain that flares with stairs, kneeling, or a long walk. Many patients accept it as a fixed sentence. The joint is wearing out, the thinking goes, so the only options are painkillers now and a replacement later.
That framing misses most of what actually helps. Research consistently indicates that the structural state of a knee on X-ray correlates poorly with how much pain a person feels. Two people with identical imaging can have very different function, and the difference usually comes down to muscle strength, body weight, activity patterns, and how the surrounding joints share the load. None of those are fixed. A coordinated plan that addresses several at once tends to outperform any single treatment, which is the case for handling osteoarthritis across disciplines rather than with one tool.
What osteoarthritis is, and what it is not
Osteoarthritis is often described as wear and tear, but that phrase is misleading. The joint is not a tire passively grinding down. It is living tissue that responds to load, and the disease involves the whole joint: cartilage, the underlying bone, the lining, the ligaments, and the muscles that control movement. Inflammation plays a role, which is why some patients feel warmth and swelling during flares rather than just mechanical stiffness.
The practical consequence is that the joint adapts to how it is used. Cartilage has limited capacity to repair, but the surrounding system has a great deal of capacity to change. Stronger muscles absorb force that would otherwise hit the joint surface. Better movement patterns distribute load more evenly. Lower body weight reduces the peak forces crossing the knee with every step. These are the levers that shift symptoms.
It also means osteoarthritis is rarely a single-knee problem. The hip above and the foot below influence how the knee tracks. A patient with weak hip muscles or a collapsed arch often loads the inner knee harder than it was built for. Assessing only the painful joint tends to miss the chain that produced the pain.
Why a single treatment usually plateaus
The default path is an anti-inflammatory and the advice to rest. Anti-inflammatories can reduce pain during a flare, and for some patients they are a reasonable part of the plan, but they treat the symptom rather than the load on the joint. Rest, taken too far, weakens the very muscles that protect the knee, which can leave a patient more vulnerable when they return to activity.
Injections, braces, and supplements each help certain patients, but they share the same limitation when used alone: they address one piece of a multi-part problem. Evidence indicates that the interventions with the strongest and most durable effect on knee osteoarthritis are exercise therapy and weight management, precisely the pieces a quick prescription cannot deliver. Patients who feel their medication stopped working have often hit the ceiling of what one lever can do.
The role of physiotherapy and movement
Exercise therapy is the most evidence-supported intervention for knee osteoarthritis, and a physiotherapist builds it around the individual joint rather than a generic handout. The aim is to strengthen the quadriceps, glutes, and hip stabilizers so the muscles share more of the load, while improving range of motion and the way the patient moves through a step or a squat.
Patients sometimes worry that loading a painful joint will damage it further. For most osteoarthritic knees the opposite is true: appropriately graded loading is what keeps cartilage and bone healthy and muscles strong. The skill is in the dosing. A good program starts where the joint can tolerate it and progresses slowly, using a simple rule that a manageable ache during and shortly after exercise is acceptable, while sharp pain or swelling that lingers into the next day means the load was too high.
Low-impact options carry most of the benefit with less joint stress. Stationary cycling, swimming, and water-based exercise build strength and endurance while the water or the bike takes the impact out. For many Calgary patients, a winter of pool work followed by graded outdoor walking in summer is a realistic year-round structure.
Where chiropractic and manual therapy fit
Manual therapy is not a treatment for the cartilage itself, and it is worth being honest about that. What it can address is the surrounding restriction that amplifies knee symptoms: a stiff hip, a locked-up ankle, or compensations through the low back that change how a person walks. When those adjacent areas move better, the knee often gets an easier job.
A chiropractor or manual therapist working within an integrated team typically focuses on improving mobility in the joints above and below, releasing tight soft tissue, and helping the patient move with less guarding. Patients commonly report that hands-on work reduces stiffness enough to make their exercise program more tolerable, which matters because the exercise is doing the structural work. The manual therapy is a way to make the active rehabilitation possible, not a substitute for it.
Weight, nutrition, and the inflammatory picture
Body weight is one of the most powerful and most underused levers in knee osteoarthritis. The forces crossing the knee during walking are several times body weight, so even a modest reduction translates into a meaningful drop in joint load with every step. Research suggests that combining weight loss with exercise produces better outcomes than either approach on its own.
A registered dietitian helps make that sustainable rather than punishing. The work is less about a restrictive diet and more about steady, livable changes that a patient can hold for years. Several dietary factors also influence the inflammatory side of osteoarthritis.
- Protein adequacy. Maintaining muscle while losing fat requires enough protein, which matters because muscle is the joint’s protection. Under-eating protein during weight loss can leave the knee weaker, not stronger.
- Omega-3 intake. Evidence indicates that omega-3 fatty acids have an anti-inflammatory effect that may help some patients with joint symptoms, and most Calgary diets are low in them.
- Overall dietary pattern. A pattern rich in vegetables, whole foods, and fish, with less ultra-processed food and added sugar, is associated with lower systemic inflammation.
- Vitamin D status. Many Calgary adults run low through the winter, and adequate vitamin D supports muscle and bone, both relevant to joint health.
The point is not a perfect diet. It is a small number of changes a patient can actually keep, layered onto the strength work, so the two reinforce each other.
Activity modification and pacing
Living well with osteoarthritis usually means adjusting how an activity is done rather than abandoning it. A patient who loves hiking does not have to stop hiking. Poles to offload the descent, shorter routes during a flare, better footwear, and a gradual build in distance often keep the activity in the patient’s life. The same logic applies to gardening, golf, and the demands of a physical job.
Pacing protects against the boom-and-bust cycle, where a patient overdoes it on a good day and then loses three days to a flare. Spreading effort across the week, alternating harder and easier days, and respecting the next-day swelling signal all keep the joint progressing rather than oscillating. Heat before activity to loosen the joint and ice after a flare are simple, low-cost tools many patients find useful.
Footwear and surfaces matter more than people expect. Cushioned, supportive shoes reduce impact, and choosing softer walking surfaces where possible takes load off the joint. For patients with a specific alignment issue, an assessment can determine whether an orthotic or a brace would help redistribute force away from the affected part of the knee.
Coordinated care for a multi-part problem
Knee osteoarthritis responds best to a plan that works on several fronts at once: stronger muscles, better movement, lower joint load, an anti-inflammatory dietary pattern, and smart pacing of the activities a patient wants to keep. No single one of these is dramatic on its own. Combined, they often change the trajectory of a joint that a patient assumed was only going to get worse.
The advantage of a setting where a physiotherapist, a chiropractor, and a registered dietitian work from the same chart is that the pieces fit together rather than competing. The exercise program, the manual therapy, and the nutrition plan reinforce one another, and the patient is not left to coordinate separate opinions. Patients with persistent or worsening knee pain should consult a qualified clinician for an individualized assessment, and those ready to address it from several angles can book an integrated joint assessment in Calgary to start.
About the author — this article was contributed by the team at Primaris Health, a Calgary multidisciplinary clinic where physiotherapists, chiropractors, and registered dietitians share one chart to build integrated care plans. The clinic supports patients managing osteoarthritis and other chronic joint conditions through coordinated movement, manual therapy, and nutrition.